The following is not FACTUALLY accurate. Details have been changed, things deleted, stuff made up, all to protect identity. But it is 100% absolutely true
Cursing the lack of windows to myself, I stole a quick glance at my phone to discern the time. A lack of any sort of circadian rhythm made anticipation of sleep, knowledge of time, or whether it was time to eat impossible. 3:30 am. Gee, I'm sure the patient will love getting a visit at this time of the night. Another service had beat me to ruining any chance of the patient or myself getting any sleep. Radiology had taken her to get an ultrasound.
I plopped down into a chair and looked over her chart in more detail. She complained of abdominal pain. ER departments love their CT scanners so she had already received the massive dose of radiation to confirm what a simple abdominal exam and labs already told us. She had appendicitis. Now the ultrasound came back and showed a goodly sized gallstone causing more trouble by backing up her pancreas. Poor lady. Got a two-for-one deal. Appendicitis AND gallstone pancreatitis. And I learned most everything I ever needed to know about an acute abdominal exam in one fell swoop. Bad for her but good for me. Such is the way of things in my training.
That was only the half of it. I would find out a day later that patients don't get a two for one without some sacrificial payment. I was regaling the valuable learning experience to another student when the resident stopped me. "Didn't you hear? She had metastatic colon cancer." An ice cold feeling dropped through my body. She had metastatic colon cancer and her belly was rebelling against the tumors. Poor lady indeed. she probably had 6 months to live. And I was reminded again of Prometheus. But this time in a poem by the German author Goethe. In it, Prometheus angrily chides the heavenly Zeus over the treatment of humanity.
COVER thy spacious heavens, Zeus,
With clouds of mist,
And, like the boy who lops
The thistles' heads,
Disport with oaks and mountain-peaks,
Yet thou must leave
My earth still standing;
My cottage too, which was not raised by thee;
Leave me my hearth,
Whose kindly glow
By thee is envied.
I know nought poorer
Under the sun, than ye gods!
Ye nourish painfully,
With sacrifices
And votive prayers,
Your majesty:
Ye would e'en starve,
If children and beggars
Were not trusting fools.
While yet a child
And ignorant of life,
I turned my wandering gaze
Up tow'rd the sun, as if with him
There were an ear to hear my wailings,
A heart, like mine,
To feel compassion for distress.
Who help'd me
Against the Titans' insolence?
Who rescued me from certain death,
From slavery?
Didst thou not do all this thyself,
My sacred glowing heart?
And glowedst, young and good,
Deceived with grateful thanks
To yonder slumbering one?
I honour thee! and why?
Hast thou e'er lighten'd the sorrows
Of the heavy laden?
Hast thou e'er dried up the tears
Of the anguish-stricken?
Was I not fashion'd to be a man
By omnipotent Time,
And by eternal Fate,
Masters of me and thee?
Didst thou e'er fancy
That life I should learn to hate,
And fly to deserts,
Because not all
My blossoming dreams grew ripe?
Here sit I, forming mortals
After my image;
A race resembling me,
To suffer, to weep,
To enjoy, to be glad,
And thee to scorn,
As I!
April 25, 2013
April 22, 2013
prometheus
The following is not FACTUALLY
accurate. Details have been changed, things deleted, stuff made up, all to
protect identity. But it is 100% absolutely true.
A falcon floated by the window behind the patient, 28 stories above the earth inside the medical tower. He had developed an inclination to look off while thinking heavily upon the right words to convey complexity to patients. He had also developed, though unbeknownst to him at the time, a proclivity of parceling out his brain. A mechanism of coping, if you will. The ability to run emotions in the background and he had plenty of those, while his ears still heard and his brain still recorded and interpreted what the patient said.
And that falcon caught and held his attention. Such a beautiful bird of prey. Was it a peregrine falcon? His eyes had faded enough with age, or the thick window distorted the waves of light enough to prevent him from discerning the identity of the bird. It glided and drifted with the updrafts, it's keen eyes constantly scanning the park below for signs of prey. Such purposeful flight. He envied the bird. A falcon is a predator and no question remains to its nature. He was not so lucky. His nature had been upended in more ways than he cared to consider. That lack of purpose made it progressively more arduous to continue to see patients.
Or perhaps, it was the confusion of purpose. The image of the bird of prey brought to mind the tale of Prometheus who stole fire from the gods and was rewarded with having an eagle eat his liver day after day, only to have the liver grow back again. Yes, he could empathize with Prometheus, while he continued to record the patient's story. He had learned how to treat the most difficult of pain, how to care for the most emotionally difficult patient, how to help someone die, and he was rewarded with having his guts devoured daily, at least figuratively, if not literally judging from the feelings of a growing pit in his stomach.
While he continued to watch the falcon, the patient concluded their story and looked expectantly at him. "Let me do a brief physical and see what we see," he told the elderly man.
"First, let me see you walk across the room," the patient gave him a bit of a smart assed scoff as if to wonder at the knowledge level of the medical student.
"Now, walk like me," he said, demonstrating the heel-toe-heel drunk walk that cops often use to assess field sobriety. The patient went from skepticism to surprise as he couldn't do it. At all. The falcon had floated from the field of view offered by the wide window. It disappointed him and left him wanting. He wanted one more good glimpse at the bird.
"Now, hop on the table and let me look at your reflexes." The patient just about came off the table. He performed a few more relevant neurologic assessments, just to be thorough, but the fore brain was starting to demand more attention from his consciousness. The emotions which ran in the background, had to shut off, at least for the benefit of the patient. But did they, he wondered? He had subsided his pain so many times before, he wondered what would happen if he no longer put the patient up first. After all, there was a doctor here to follow up on him. To make sure he didn't miss anything. What would it hurt?
In the end, his pride figured into the equation. He wanted to find something the doctor didn't. And nothing trivial, either. This patient likely had cervical myelopathy. And in the end, he genuinely did wish to help the patient despite the upsetting of that delicate balance between his emotions and his cognition. It seemed so very fragile. A line in the sand was drawn, separating his well-being from the patient's well-being, and whether it was the 100th or 10,000th time, it didn't seem to matter anymore. He couldn't possibly let this patient walk out with a missed diagnosis of cervical myelopathy.
Turning his back on the window and the now absent hawk, he left the room and told the attending doc his suspicions. The attending listened and looked at him quizzically. Did the attending believe him? The attending believed enough to verify the findings. "Let me see your reflex hammer," as surgeons they don't ask, they demand. When the patient gave a repeat performance, the attending looked at the medical student with an arched eyebrow. The attending was impressed, he could tell. Would that newly earned respect still be there if it was known that below the surface, he struggled daily to keep himself together? That every time he saw someone with cancer, with pain, with a deadly illness, his already broken heart and psyche fell apart that much more? But he didn't really care what attendings thought anymore. He had done right by the patient and he had done right by himself. That was all that mattered and now it was time for the emotions to regain their grip on his thoughts.
A falcon floated by the window behind the patient, 28 stories above the earth inside the medical tower. He had developed an inclination to look off while thinking heavily upon the right words to convey complexity to patients. He had also developed, though unbeknownst to him at the time, a proclivity of parceling out his brain. A mechanism of coping, if you will. The ability to run emotions in the background and he had plenty of those, while his ears still heard and his brain still recorded and interpreted what the patient said.
And that falcon caught and held his attention. Such a beautiful bird of prey. Was it a peregrine falcon? His eyes had faded enough with age, or the thick window distorted the waves of light enough to prevent him from discerning the identity of the bird. It glided and drifted with the updrafts, it's keen eyes constantly scanning the park below for signs of prey. Such purposeful flight. He envied the bird. A falcon is a predator and no question remains to its nature. He was not so lucky. His nature had been upended in more ways than he cared to consider. That lack of purpose made it progressively more arduous to continue to see patients.
Or perhaps, it was the confusion of purpose. The image of the bird of prey brought to mind the tale of Prometheus who stole fire from the gods and was rewarded with having an eagle eat his liver day after day, only to have the liver grow back again. Yes, he could empathize with Prometheus, while he continued to record the patient's story. He had learned how to treat the most difficult of pain, how to care for the most emotionally difficult patient, how to help someone die, and he was rewarded with having his guts devoured daily, at least figuratively, if not literally judging from the feelings of a growing pit in his stomach.
While he continued to watch the falcon, the patient concluded their story and looked expectantly at him. "Let me do a brief physical and see what we see," he told the elderly man.
"First, let me see you walk across the room," the patient gave him a bit of a smart assed scoff as if to wonder at the knowledge level of the medical student.
"Now, walk like me," he said, demonstrating the heel-toe-heel drunk walk that cops often use to assess field sobriety. The patient went from skepticism to surprise as he couldn't do it. At all. The falcon had floated from the field of view offered by the wide window. It disappointed him and left him wanting. He wanted one more good glimpse at the bird.
"Now, hop on the table and let me look at your reflexes." The patient just about came off the table. He performed a few more relevant neurologic assessments, just to be thorough, but the fore brain was starting to demand more attention from his consciousness. The emotions which ran in the background, had to shut off, at least for the benefit of the patient. But did they, he wondered? He had subsided his pain so many times before, he wondered what would happen if he no longer put the patient up first. After all, there was a doctor here to follow up on him. To make sure he didn't miss anything. What would it hurt?
In the end, his pride figured into the equation. He wanted to find something the doctor didn't. And nothing trivial, either. This patient likely had cervical myelopathy. And in the end, he genuinely did wish to help the patient despite the upsetting of that delicate balance between his emotions and his cognition. It seemed so very fragile. A line in the sand was drawn, separating his well-being from the patient's well-being, and whether it was the 100th or 10,000th time, it didn't seem to matter anymore. He couldn't possibly let this patient walk out with a missed diagnosis of cervical myelopathy.
Turning his back on the window and the now absent hawk, he left the room and told the attending doc his suspicions. The attending listened and looked at him quizzically. Did the attending believe him? The attending believed enough to verify the findings. "Let me see your reflex hammer," as surgeons they don't ask, they demand. When the patient gave a repeat performance, the attending looked at the medical student with an arched eyebrow. The attending was impressed, he could tell. Would that newly earned respect still be there if it was known that below the surface, he struggled daily to keep himself together? That every time he saw someone with cancer, with pain, with a deadly illness, his already broken heart and psyche fell apart that much more? But he didn't really care what attendings thought anymore. He had done right by the patient and he had done right by himself. That was all that mattered and now it was time for the emotions to regain their grip on his thoughts.
April 19, 2013
suicide
I've been thinking about suicide a lot lately. No, not in that way. I've had several patients lately who have either been severely depressed or outright suicidal. That would be normal if I was still on my psych rotation. But these were surgical patients. It got me to pondering the dilemma of the suicidal impulse. I first looked through the literature, at least as it will pertain to me going into family practice. It turns out we do a pretty poor job of identifying and treating depression, never mind suicidal patients. No surprises there. If we were good at it, then I suspect the suicide rate wouldn't be double the homicide rate. So I instead turned to the writings of those who had either pondered or followed through the act of ending one's own life. This excerpt from the internet genius, but now deceased Aaron Swartz is pretty descriptive into what those tortured souls must feel.
Depressed mood: Surely there have been times when you’ve been sad. Perhaps a loved one has abandoned you or a plan has gone horribly awry. Your face falls. Perhaps you cry. You feel worthless. You wonder whether it’s worth going on. Everything you think about seems bleak — the things you’ve done, the things you hope to do, the people around you. You want to lie in bed and keep the lights off. Depressed mood is like that, only it doesn’t come for any reason and it doesn’t go for any either. Go outside and get some fresh air or cuddle with a loved one and you don’t feel any better, only more upset at being unable to feel the joy that everyone else seems to feel. Everything gets colored by the sadness.
At best, you tell yourself that your thinking is irrational, that it is simply a mood disorder, that you should get on with your life. But sometimes that is worse. You feel as if streaks of pain are running through your head, you thrash your body, you search for some escape but find none. And this is one of the more moderate forms. As George Scialabba put it, “acute depression does not feel like falling ill, it feels like being tortured … the pain is not localized; it runs along every nerve, an unconsuming fire. … Even though one knows better, one cannot believe that it will ever end, or that anyone else has ever felt anything like it.”
The economist Richard Layard, after advocating that the goal of public policy should be to maximize happiness, set out to learn what the greatest impediment to happiness was today. His conclusion: depression. Depression causes nearly half of all disability, it affects one in six, and explains more current unhappiness than poverty. And (important for public policy) Cognitive-Behavioral Therapy has a short-term success rate of 50%. Sadly, depression (like other mental illnesses, especially addiction) is not seen as “real” enough to deserve the investment and awareness of conditions like breast cancer (1 in 8) or AIDS (1 in 150). And there is, of course, the shame.
April 18, 2013
concerns
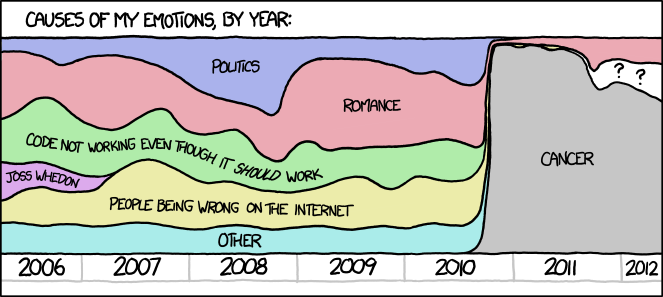
From the web comic xkcd, this kind of honesty can only come from someone who intimately knows cancer.
April 15, 2013
sum of the parts
The following is not FACTUALLY
accurate. Details have been changed, things deleted, stuff made up, all to
protect identity. But it is 100% absolutely true.
Pain, both physical and emotional, were overwhelming the patient. A victim of a nasty trauma, the patient had injuries to both the cervical and lumbar vertebrae, not to mention the spine. The patient's injuries inflicted pain when the sun rose, and pain when the sun set. Pain was never absent. I could tell this interview needed to be directed towards a darker area, despite the fact that I was on my surgery rotation and as one attending told me, "I'm not a *%)$*#( psychiatrist. Focus on the wound."
But being an older student, I'm more concerned with learning how to be a good doc, not on getting a good grade. Sadly, there exists a massive chasm between being a good student and a good doc. They are not necessarily one and the same. So I gently asked the patient about suicide. Without any surprise, the patient confirmed what I already knew. Loss of physical vitality, loss of livelihood, loss of sleep, loss of hope coupled with ever present pain is enough to drive the most resilient of person to consider the notion of "opting out". For all the talk and hype surrounding murders in this country of late, suicide destroys far more lives than homicide (twice as many, in fact). I have no idea if the patient solicited the help to which they were referred. I have no idea if their pain was ever brought under control enough to enjoy life again. It's on one of the reasons I want to go into Family Medicine. I want to know the whole patient's story, not just one specific problem.
Pain, both physical and emotional, were overwhelming the patient. A victim of a nasty trauma, the patient had injuries to both the cervical and lumbar vertebrae, not to mention the spine. The patient's injuries inflicted pain when the sun rose, and pain when the sun set. Pain was never absent. I could tell this interview needed to be directed towards a darker area, despite the fact that I was on my surgery rotation and as one attending told me, "I'm not a *%)$*#( psychiatrist. Focus on the wound."
But being an older student, I'm more concerned with learning how to be a good doc, not on getting a good grade. Sadly, there exists a massive chasm between being a good student and a good doc. They are not necessarily one and the same. So I gently asked the patient about suicide. Without any surprise, the patient confirmed what I already knew. Loss of physical vitality, loss of livelihood, loss of sleep, loss of hope coupled with ever present pain is enough to drive the most resilient of person to consider the notion of "opting out". For all the talk and hype surrounding murders in this country of late, suicide destroys far more lives than homicide (twice as many, in fact). I have no idea if the patient solicited the help to which they were referred. I have no idea if their pain was ever brought under control enough to enjoy life again. It's on one of the reasons I want to go into Family Medicine. I want to know the whole patient's story, not just one specific problem.
April 8, 2013
sewing
The following is not FACTUALLY
accurate. Details have been changed, things deleted, stuff made up, all to
protect identity. But it is 100% absolutely true.
The trauma page went over head as I followed my chief resident into the critical care unit. It turns out that pointy sharp objects and skin don't mix very well. Her skilled fingers guided by experience and talent quickly located the vein bleeding and tied it off. What was left behind was a large bloody mess. She turned to me and asked, "can you handle the rest?"
"The rest" meaning clean up and put this gash back together.

There is a definite appeal to surgery. The patient's problem is (usually) clearly defined and amenable to physical alterations. If it wasn't, the patient wouldn't be in surgery. Consequently, surgeons tend to be very cut and dry, very goal oriented. Subtlety is not in their vocabulary. It's also instant gratification. All bleeding stops eventually, so you know if you saved the patient in relatively short time. Nothing like primary care where you're treating chronic life long conditions like diabetes.
While I have ZERO interest in going into surgery, I can admit it was a nice change of pace to just focus on the mechanical task at hand by sewing up the wound. It's not the prettiest job ever but the chief wanted to leave it open somewhat to allow some drainage. Now I'm definitely ready the next time my son decides to play with something sharp. No more going to the ER for him. Dad's giving him a shot of tequila and sewing him up.

The trauma page went over head as I followed my chief resident into the critical care unit. It turns out that pointy sharp objects and skin don't mix very well. Her skilled fingers guided by experience and talent quickly located the vein bleeding and tied it off. What was left behind was a large bloody mess. She turned to me and asked, "can you handle the rest?"
"The rest" meaning clean up and put this gash back together.

There is a definite appeal to surgery. The patient's problem is (usually) clearly defined and amenable to physical alterations. If it wasn't, the patient wouldn't be in surgery. Consequently, surgeons tend to be very cut and dry, very goal oriented. Subtlety is not in their vocabulary. It's also instant gratification. All bleeding stops eventually, so you know if you saved the patient in relatively short time. Nothing like primary care where you're treating chronic life long conditions like diabetes.
While I have ZERO interest in going into surgery, I can admit it was a nice change of pace to just focus on the mechanical task at hand by sewing up the wound. It's not the prettiest job ever but the chief wanted to leave it open somewhat to allow some drainage. Now I'm definitely ready the next time my son decides to play with something sharp. No more going to the ER for him. Dad's giving him a shot of tequila and sewing him up.

April 1, 2013
birthday present
Usually, it begins with a phone call. But this time it started with a voice mail. From my dad, he had some questions about his recent CT scan. One of the quirks at MDACC is that the patient will oftentimes have the reports to various tests - CT scans, biopsies, blood draws, whatever - posted to their online account before they've met with their oncologist. And though my dad's bone marrow biopsy, his molecular assessment and all that it entails (I'm not going into the details), and his blood work showed that he was 100% engrafted and 100% in remission, there were two little sentences in his thoracic CT which were reason for pausing. Not even full sentences, really. Just two measly statements out of multiple boring ones:
"It could be a lot of things. Seeing as how you recently had a respiratory infection, it's likely that it's just a hold over from that bug you had," I said.
"What else could it be? The radiologist wouldn't be recommending follow up unless there were other possibilities." I could see my dad's mental faculties were still intact.
Taking a pause while remembering a similar conversation I had with my dad about two years ago when he was first being diagnosed, I asked him, "do you really want to go down that road just yet?" He did. So we had the conversation about the possibility of another malignancy. Thoughts of more testing, more chemotherapy, more fighting.....It's more than one person would care to endure.
It's likely the finding is the remnants of his recent infection. It's less likely to be cancer. But not improbable. The price of surviving cancer is eternal vigilance.
There is a new 0.7 x 0.5 cm poorly marginated nodular opacity in the right lower lobe posteriorly (image 95 of series 4). This may be a postinflammatory focus and recommend short-term followup (sic) to ensure stability or resolution.Just simply uttering the word "new" to a cancer patient is reason enough cause them to hold their breath in worried anticipation. And "poorly marginated" are buzzwords to clinicians. They normally do not imply benign findings. And so my dad asked me what the report meant.
"It could be a lot of things. Seeing as how you recently had a respiratory infection, it's likely that it's just a hold over from that bug you had," I said.
"What else could it be? The radiologist wouldn't be recommending follow up unless there were other possibilities." I could see my dad's mental faculties were still intact.
Taking a pause while remembering a similar conversation I had with my dad about two years ago when he was first being diagnosed, I asked him, "do you really want to go down that road just yet?" He did. So we had the conversation about the possibility of another malignancy. Thoughts of more testing, more chemotherapy, more fighting.....It's more than one person would care to endure.
It's likely the finding is the remnants of his recent infection. It's less likely to be cancer. But not improbable. The price of surviving cancer is eternal vigilance.
Subscribe to:
Posts (Atom)